

Editor’s note: This article is part of PRF’s featured content series, “Investigating Virtual Reality for Pain Management: Past, Present, and Future,” which has been made possible thanks to a generous grant from the MAYDAY Fund.
Virtual reality (VR) creates immersive and interactive computer-generated environments designed to replace real-world sensory inputs. VR users typically experience these environments through headsets or goggles, and the nature of these VR environments can distract the user from what is happening in the environment around them. Distraction has long been used as a technique to help manage pain, so it is unsurprising to learn that VR is being used to help manage both acute and chronic pain. As this technology evolves, however, we’re learning that there are more mechanisms at play than simply distraction.
The first recorded study using VR in the context of pain management was published back in 2000, led by Hunter Hoffman (University of Washington, USA). Hoffman and his colleagues used VR as a means for adjunctive pain control during wound care procedures in adolescent patients with burn injuries.
The idea to use VR came about through discussions between Hoffman and his friends and longtime collaborators John Everett and David Patterson.
“I was having a conversation with John [Everett] – my friend who I went to graduate school with – and he was telling me about his dissertation with David Patterson using hypnosis for pain control in burn patients,” Hoffman recalled.
“I asked John about how hypnosis reduced pain, and he explained that it wasn’t well understood but that it may have something to do with distraction. I’d been working with VR prior to that, so when he mentioned distraction I thought, ‘Oh gosh, I’ve got a distraction that will knock your socks off.’
“So we went out for a beer and John introduced me to Dave, who thought using VR sounded like a no-brainer that could be really valuable. It took a couple of years [after that], but we eventually started collaborating.”
In their initial study (Hoffman et al., 2000), Hoffman and Patterson used a VR system to distract two teenage patients from their acute pain associated with burn wound care procedures. Specifically, the patients experienced SpiderWorld, where they could “physically touch” the furry body of a virtual tarantula.
These initial cases reported dramatic reductions in pain and anxiety during the wound care procedures when VR was utilized, but despite its effectiveness, SpiderWorld wasn’t perfect.
Turning to the land of ice and snow
SpiderWorld wasn’t very popular [with patients], even though it was very effective,” said Hoffman. “The patients felt a need for there to be something other than spiders, because experiencing the wound care was already unpleasant enough.”
Based on this feedback, Hoffman informally surveyed patients, nurses, and his colleagues to get a better understanding of what wound care was like.
“Several of them said wound care was like being burned again. Many patients’ thoughts turned to images of burning cars during the wound care procedures. It became clear that spiders were bad, but fire was worse.”
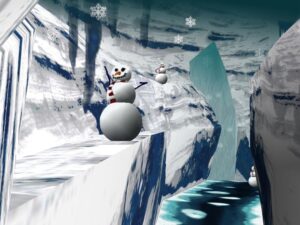
This feedback led Hoffman and his colleagues to develop SnowWorld, an icy VR environment designed to contrast fire and burns. In SnowWorld, patients can throw snowballs at an endless parade of penguins lining a wintery canyon by clicking a mouse button, or simply sit back and enjoy the ride.
“SnowWorld was designed specifically to put out the fires of their burn pain,” explained Hoffman. “The colors were specifically designed to be a lot of blues, whites, and greens – no reds or oranges.”
Perhaps the most unique aspect of SnowWorld, however, is its soundtrack: Paul Simon’s Graceland. Hoffman has fond memories of his encounters with Paul Simon over the past two decades.
“Paul was on tour, and one of his buddies recommended he come and visit the Human Interface Technology lab when he made it to Seattle. We had 10 different things set up for him to try, because we wanted to impress him,” said Hoffman.
“He arrived late, so I thought I’d give him the short[er] version of the tour instead, but he insisted on getting the full tour. I showed him SnowWorld – which at the time had sound effects but not music – and he suggested we could use Graceland if we wanted.”
While initially unsure of Simon’s offer, Hoffman’s now thrilled the opportunity arose.
“I wasn’t sure if it would be the most appropriate music, as it’s a contradiction. SnowWorld is very ‘arctic’ and ‘Christmassy,’ while Graceland features a few South African styles of music, which might lead you to think of hot or warm things.
“But it has a nice beat and appeals to a very wide audience. We’ve used it with children through people in their eighties, and it makes you feel good.”
Graceland is still used as backing music for SnowWorld to this day.
Beyond distraction
Following the success of using VR as a non-pharmacological alternative for the pain associated with burn wound care, VR has proven to be effective in other pain-related conditions, including dental pain (Hoffman et al., 2001), physiotherapy-associated pain in cerebral palsy (Steele et al., 2003), transurethral microwave thermotherapy (Wright et al., 2005), and venipuncture (Atzori et al., 2018).
Imaging research has also proven that VR reduces pain-related brain activity. In a 2004 study, Hoffman and colleagues compared pain-related brain activity – with and without the use of VR technology – when participants were exposed to a thermal pain stimulus while undergoing an fMRI scan (Hoffman et al., 2004). In addition to reducing all subjective pain reports, VR also reduced pain-related brain activity in five regions of interest: The anterior cingulate cortex, the primary and secondary somatosensory cortex, the insula, and the thalamus.
The use of VR for chronic pain management has received significant interest, and more studies are now showing that this pain relief may be more than just distraction based. In a 2023 study, distinct neural mechanisms – as measured through 32-channel electroencephalography – were shown to be responsible for VR-induced analgesia (Li et al., 2023), particularly in spontaneous alpha and gamma oscillations. Similarly, EEG studies investigating the effect of VR on cortical processing of evoked potentials have shown that active participation in VR decreased pre-perceptual and perceptual brain activity following painful electrical stimuli, corresponding to the reduced experience of pain (Lier et al., 2020).
One chronic pain symptom of particular interest to VR researchers is somatic disperception – the loss of the ability to accurately map body parts perceiving chronic pain, thus manipulating how the body is perceived. This can be seen in patients with phantom limb pain, chronic low-back pain, and complex regional pain syndrome (Alemanno et al., 2019). One such researcher, Daniel Harvie – a physiotherapist, pain scientist, and educator from the University of South Australia – has focused on investigating new approaches to chronic pain management, particularly those that leverage exploratory technologies and modern understandings of sensory processing. Naturally, Harvie has used VR as a part of his chronic pain research program for more than a decade.
One of Harvie’s first forays into this area involved using VR to test whether manipulating visual proprioception cues could alter movement-related pain in people with chronic neck pain (Harvie et al., 2015).
To do this, Harvie and his colleagues used VR to manipulate the rotational gain – how much real rotation is translated to virtual rotation – when people turned their head and neck from side to side under a series of different conditions. One condition overstated the displayed rotation on the VR headset (compared to how much their neck actually moved), while another condition displayed the same amount of rotation, and the final condition understated the displayed rotation on the headset.
When the VR informed patients that they had moved their head farther than they did in the physical world, they reported feeling pain earlier compared to the control condition. In contrast, when the patients received feedback that they had moved their head a smaller amount than what they actually did, they reported feeling pain at a later point.
Challenges remain in identifying optimal VR use
More recently, Harvie published a clinical note of his experiences using VR to explore touch-evoked pain in a patient with long-standing complex regional pain syndrome (Harvie et al., 2022). The touch-evoked pain was so extreme for the patient that even touching things in a virtual environment – without any physical contact – resulted in pain.
To address this response, Harvie and his colleagues developed a 12-week VR graded exposure program. The graded exposure ranged from mild, like running the hand under a virtual stream of water, to extreme, such as stabbing a virtual barbecue poker through the hand. The touch-evoked pain had almost been completely extinguished by the end of the 12 weeks.
“At the end of 12 weeks, he was repeatedly stabbing himself with this barbecue poker [for] up to 70 seconds before he got any pain at all,” Harvie told The Knowledge Exchange Podcast. “We also assessed the clinical effects outside of VR, and it had [no effect].”
Harvie is keen to use the lack of real-world findings to enhance our understanding of how pain works, and the challenges of trying to translate VR-based effects into real-world improvements.
“[The lack of real-world findings] also says something like treatments that we apply in one context don’t necessarily generalize to another context. So I guess as we explore this idea further, our challenge is if this idea has some clinical benefit in its future, we’re going to have to tackle this problem of how we get that effect to carry over into the real world.
“Phrases like ‘VR has been shown to be effective in low back pain’ is a complete throwaway to me because VR isn’t a treatment…. If you want to use VR as a tool for delivering that, then that’s the right way to think about it, with the caveat that you need to ask yourself ‘Can I do this better outside of VR than inside VR?’”
Things have certainly come a long way since Hoffman and Patterson first used VR to help reduce pain in burn patients. VR technology has made rapid advances in recent years, making virtual reality equipment more affordable, portable, and realistic. However, Harvie emphasizes the importance of not getting overly caught up in the new technology and remembering equivalent, physical activities. Now, new studies are investigating VR-supplemented therapies, such as interactive virtual walking to reduce neuropathic pain in spinal cord injury (Trost et al., 2022), phantom limb pain (Hoffman et al., 2020), and even women in active labor (Carus et al., 2022).
Technological advancements in the immersive nature of VR promise to open new avenues for clinical intervention and potential non-medicated and at-home treatments of various pain conditions. For now, it will be fascinating to observe how researchers and clinicians continue to identify and implement novel ways for VR to be used in the management of both acute and chronic pain in the coming years.
Lincoln M. Tracy, PhD, is a freelance science writer and researcher based in Australia.
![]()
Featured image: Virtual reality stimuli. Harvie et al., PAIN. 2022.
Inline image: An early iteration of SnowWorld. Hoffman et al., PAIN. 2004.
Related Reading
Alemanno F, Houdayer E, Emedoli D, et al. Efficacy of virtual reality to reduce chronic low back pain: Proof-of-concept of a non-pharmacological approach on pain, quality of life, neuropsychological and functional outcome. PLoS One. 2019;14(5):e0216858. Published 2019 May 23. doi:10.1371/journal.pone.0216858
Atzori B, Hoffman HG, Vagnoli L, et al. Virtual Reality Analgesia During Venipuncture in Pediatric Patients With Onco-Hematological Diseases. Front Psychol. 2018;9:2508. Published 2018 Dec 20. doi:10.3389/fpsyg.2018.02508 PMID: 30618938
Carus EG, Albayrak N, Bildirici HM, Ozmen SG. Immersive virtual reality on childbirth experience for women: a randomized controlled trial. BMC Pregnancy Childbirth. 2022;22(1):354. Published 2022 Apr 23. doi:10.1186/s12884-022-04598-y
Harvie DS, Broecker M, Smith RT, Meulders A, Madden VJ, Moseley GL. Bogus visual feedback alters onset of movement-evoked pain in people with neck pain. Psychol Sci. 2015;26(4):385-392. doi:10.1177/0956797614563339. PMID: 25691362
Harvie DS, Stanton TR, Kennedy H, Coppieters MW. Visually evoked pain and its extinction using virtual reality in a patient with complex regional pain syndrome type II. Pain. 2022 Oct 1;163(10):1874-1878. doi:10.1097/j.pain.0000000000002605. Epub 2022 Jan 31. PMID: 35297803.
Hoffman HG, Boe DA, Rombokas E, et al. Virtual reality hand therapy: A new tool for nonopioid analgesia for acute procedural pain, hand rehabilitation, and VR embodiment therapy for phantom limb pain. J Hand Ther. 2020;33(2):254-262. doi:10.1016/j.jht.2020.04.001
Hoffman HG, Doctor JN, Patterson DR, Carrougher GJ, Furness TA 3rd. Virtual reality as an adjunctive pain control during burn wound care in adolescent patients. Pain. 2000;85(1-2):305-309. doi:10.1016/s0304-3959(99)00275-4. PMID: 10692634
Hoffman HG, Garcia-Palacios A, Patterson DR, Jensen M, Furness T 3rd, Ammons WF Jr. The effectiveness of virtual reality for dental pain control: a case study. Cyberpsychol Behav. 2001;4(4):527-535. doi:10.1089/109493101750527088. PMID: 11708732
Hoffman HG, Sharar SR, Coda B, Everett JJ, Ciol M, Richards T, Patterson DR. Manipulating presence influences the magnitude of virtual reality analgesia. Pain. 2004 Sep;111(1-2):162-8. doi: 10.1016/j.pain.2004.06.013. PMID: 15327820.
Hoffman HG, Richards TL, Coda B, et al. Modulation of thermal pain-related brain activity with virtual reality: evidence from fMRI. Neuroreport. 2004;15(8):1245-1248. doi:10.1097/01.wnr.0000127826.73576.91. PMID: 15167542
Li J, Yang H, Xiao Y, et al. The analgesic effects and neural oscillatory mechanisms of virtual reality scenes based on distraction and mindfulness strategies in human volunteers. Br J Anaesth. 2023;131(6):1082-1092. doi:10.1016/j.bja.2023.09.001.
Lier EJ, Oosterman JM, Assmann R, de Vries M, van Goor H. The effect of Virtual Reality on evoked potentials following painful electrical stimuli and subjective pain. Sci Rep. 2020;10(1):9067. Published 2020 Jun 3. doi:10.1038/s41598-020-66035-4
Steele E, Grimmer K, Thomas B, Mulley B, Fulton I, Hoffman H. Virtual reality as a pediatric pain modulation technique: a case study. Cyberpsychol Behav. 2003;6(6):633-638. doi:10.1089/109493103322725405. PMID: 14756928
Trost Z, Anam M, Seward J, et al. Immersive interactive virtual walking reduces neuropathic pain in spinal cord injury: findings from a preliminary investigation of feasibility and clinical efficacy. Pain. 2022;163(2):350-361. doi:10.1097/j.pain.0000000000002348
Wright JL, Hoffman HG, Sweet RM. Virtual reality as an adjunctive pain control during transurethral microwave thermotherapy. Urology. 2005;66(6):1320. doi:10.1016/j.urology.2005.06.123. PMID: 16360473