


We all know how common back pain is and how back pain comprises a significant proportion of the 1 in 4 people with persistent pain. There is clearly an established link between the meaning of one’s pain and the fear it evokes, right? Someone’s perception of what it happening in their back relates to their pain, right? Castrophisation scales and measures of fear avoidance are about the strongest links we’ve discovered to the maintenance (if not etiology) of persistent pain, right?
Well, while perusing a colleague’s notes from a CPD course they had just done, I was struck by the section shown below. In fact, it jumped right out of the page and had me gaping!
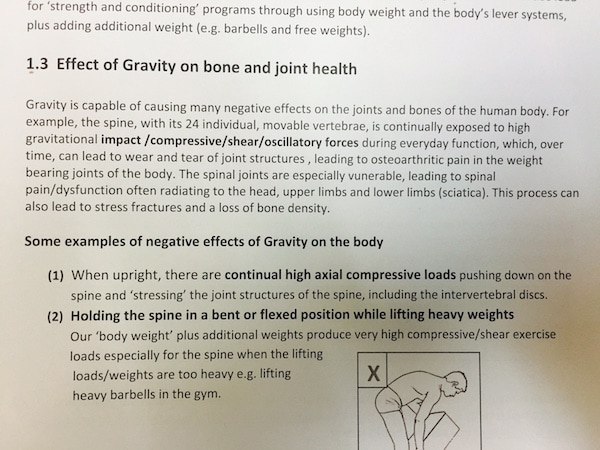
Check out the catastrophic wording of the effect of gravity on our joints and the potential for significant harm! Gravity! One might suggest that gravity is actually a vital contributor to health. One might suggest that without gravity, one’s body goes to pot – in fact, one’s brain might just go to pot too. One might suggest that the very properties that gravity moulds – critical strengthening where loads are likely (is there anything that is not outstanding about the realignment of boney trabeculae with gravitational and other forces? Was Wollf talking rubbish?) are sufficient to say that gravity is not just safe, but vital.
So, what is being achieved with such professional development? I am a very enthusiastic supporter of the value of a sound understanding of biomechanics and its potential role in injury and pain and their management. However, if we don’t train modern therapists in a paradigm that places biomechanics in a rational neuroscience (or a truly biopsychosocial) framework – then how are these therapists going to be equipped to dethreaten a person’s experience of first time LBP – their disc injury that doesn’t get better…
I wonder too, if the impact of this kind of approach to understanding and communicating biology has significant ripple effects. Does language such as that used in the material pictured, delivered as part of CPD, lead therapists to themselves catastrophize, worry and become fearful? By passing on these ideas, that are completely infused with danger cues, how do we live up to doing no harm? I suspect that those in BiM’s orbit would doubt we can, but what about those clinicians that are not in BiM’s orbit…
I am led to reflect on a family member who in conversation with me indicated that after her spinal fusion surgery she really felt quite good. In the first 6 weeks during which she was advised against physiotherapy, while her tissue healed – she walked, swam and cared for her granddaughter. She felt confident and robust. She was very functional and was glad to have had the surgery – a good result for her. Then she saw the physio, who had her do abdominal exercises in a particular way – advising her that she was doing them all wrong, that she was not protecting her back very well, and that it was vital that she learnt ‘the right strategy’. Hey presto! She began to doubt her recovery. She began to doubt her confidence and robustness. Her self-efficacy for walking, swimming and household duties – all things she had been doing well – began to fade. She reduced her walking and swimming and backed off on the housework.
In my role teaching pain sciences to undergraduate and post-graduate allied health students, I have found this conceptual conflict quite common. I am convinced that if we are to exploit all the excellent stuff our extensive biomechanical training gives us, then we simply must apply it within a wider biopsychosocial context. If we don’t then we are not being neutral bystanders in the lives and rehabilitation of our patients – we may well, in Australian parlance, ‘be stuffing them up’.
About Jeannie Burnett
 Jeannie Burnett is a physiotherapist with Masters qualification in musculoskeletal and manual therapy. She teaches pain sciences at the University of South Australia. Along with this she is involved in clinical education in Musculoskeletal placements and works in private practice. The interface between what we have learned in the pain realm and what we do in practice – really the research to clinic integration – is what really floats her boat.
Jeannie Burnett is a physiotherapist with Masters qualification in musculoskeletal and manual therapy. She teaches pain sciences at the University of South Australia. Along with this she is involved in clinical education in Musculoskeletal placements and works in private practice. The interface between what we have learned in the pain realm and what we do in practice – really the research to clinic integration – is what really floats her boat.